The conventional treatment for an amputation above the knee is a specially fitted cup-like shell called a socket. It fits over the remaining portion of the patients’ leg and helps secure the device to the leg. If patients do not have a long enough residual limb to properly fit socket prosthesis or have other conditions, such as scarring, pain, recurrent skin infections, or fluctuations in the shape of the residual limb they are just out of luck.
New Leg Prosthesis Gains FDA Approval
1 min read Premium comments
Secondary
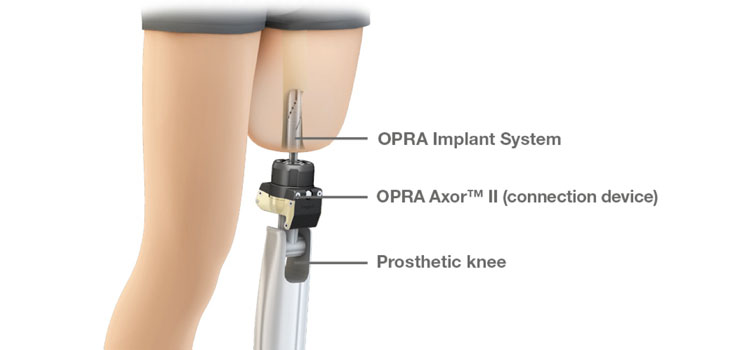
To remedy that situation the FDA has authorized the first prosthesis to be marketed in the U.S. for patients who cannot use the conventional socket prosthesis. The device is called the Osseoanchored Prostheses for the Rehabilitation of Amputees (OPRA). It uses fixtures and screws that are implanted into the patient’s remaining thigh bone to connect an external limb.
According to the FDA press release, the OPRA device is installed with two surgical procedures. In the first procedure, a cylinder-shaped fixture is implanted into the central canal of the remaining thigh bone. Approximately six months later, after tissue has grown to anchor the fixture and the skin tissue has healed, a second surgery is performed to implant a rod that attaches to the fixture from the previous surgery. This rod extends through the skin at the bottom of the patient’s residual limb and connects to the prosthetic leg.
After the second surgery, the patient works with a specially trained physical therapist to gradually place weight on the OPRA device using a training prosthesis. Patients require about six months of training and rehabilitation after the second surgery, before being fitted with their own customized prosthesis.
“Prostheses can help people who have lost a leg due to trauma or cancer to regain mobility and to more easily participate in everyday activities, ” said William Maisel, M.D., M.P.H., acting director of the Office of Device Evaluation in the FDA’s Center for Devices and Radiological Health. “The OPRA device may help those with above-the-knee amputations who have had problems with rehabilitation and have not been able to benefit from available socket prostheses.”
The OPRA device is manufactured by Integrum AB in Molndal, Sweden.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.