The American Academy of Orthopaedic Surgeons (AAOS) is attempting to help surgeons when the pressure is really on in the OR. If you need to treat a child with elbow fractures where there is a vascular injury involved, you can now benefit from AAOS guidelines. The Appropriate Use Criteria (AUC) walks surgeons through the assessment and treatment of this condition, which, according to AAOS, if not treated quickly and appropriately, can result in permanent damage and loss of function in the arm and hand. The AUC for supracondylar humerus fractures with vascular injury is available on the Academy’s website, and through the OrthoGuidelines mobile app.
AAOS: New Guidelines for Child Elbow Fractures With Vascular Injury
2 min read Premium comments
Secondary
“When physicians face one of these cases, which may be once in a blue moon, it can be uncomfortable deciding what the next steps should be, ” said James O. Sanders, M.D., former chair of AAOS AUC within the Committee on Evidence-Based Quality and Value, in the June 24, 2015 news release. “These criteria are really meant to help doctors in the heat of the moment. No one sees enough of these to become a true expert in how to deal with them.”
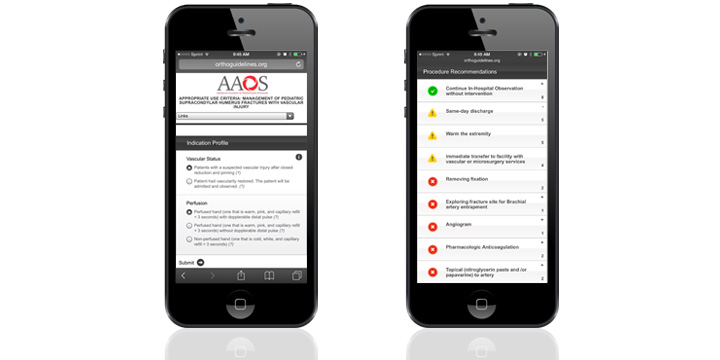
According to the news release, “Depending on the patient’s vascular status and perfusion, the orthopaedist is directed to next steps and possible interventions. For example, if the child has a suspected vascular injury after the fracture has been pinned and set, but the hand is warm and red with a pulse, in-hospital observation is recommended without intervention. In all situations where the hand is without a pulse, the criteria recommend that the child be assessed by a vascular surgeon, or immediately transferred to a facility with such expertise. If the hand is white without a pulse, the AUC recommends consideration of removing the fixation and possibly obtaining an angiogram.”
Dr. Sanders told OTW, “The typical orthopedist has struggled with these injuries and most often attempted to get them to regional children’s trauma centers promptly. Even at these centers, having some basic protocols has been difficult because the literature is not clear on exactly what should be done.”
Asked the points in the decision making process where things can go wrong, Dr. Sanders noted, “There are lots of places care can go wrong. The child can be treated in a hospital without the needed service, and the rare problem then becomes a disaster for the patient. The vessel can get stuck in the fracture site and the surgeon does not remove it. Just as airplane pilots use checklists in emergencies to help them function well despite knowing all the proper steps, surgeons face similar situations, and the AUC is designed to help those of us in these situations to properly consider the important options.”
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.