Infections and their treatment are on the mind of every orthopedic surgeon. New work from scientists at Thomas Jefferson University and the National Institutes of Health (NIH) is giving insight into the why infections tend to be so difficult to get under control.
Infection Progress From TJU, NIH
2 min read Premium comments
Secondary
“Biofilm formation has been suspected to play a key role during septic arthritis and prosthetic joint infection.” said Noreen Hickok, Ph.D., associate professor in the Department of Orthopedic Surgery in the Sidney Kimmel Medical College at Thomas Jefferson University, in the October 2, 2014 news release.
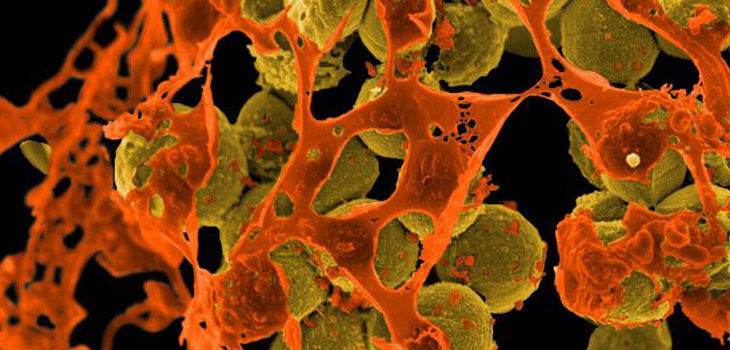
The team, also led by co-investigator is Michael Otto, Ph.D., a senior investigator with the Laboratory of Human Bacterial Pathogenesis National Institute for Allergies and Infectious Diseases, National Institutes of Health, set out to determine whether the bacteria behaved differently in the synovial fluid. After growing several strains of methicillin-resistant Staphylococcus aureus (MRSA) the team found that the “bacteria begin to grow as clumps in the synovial fluid, and that these clumps share many of the same properties as biofilms. They also found that the bacteria slow their growth, making them even less susceptible to antibiotics, which are designed to target rapidly growing cells like bacteria.”
The study, published in Journal of Infectious Diseases, indicates that the biofilm clumps could be prevented by “pre-treating the synovial fluid with a plasmin enzyme that degraded the protein matrix. With this pre-treatment, the research team reduced the formation of bio-floater clumps and increased the bacterial susceptibility to antibiotics.”
“The study also helps explain why joint infections are so difficult to diagnose, even when there are overt signs of infection, ” said Dr. Hickok.
Dr. Hickok told OTW, “The important message is that MRSA and methicillin-susceptible Staphylococcus aureus become biofilm-like as soon as they enter the synovial environment. Thus, we would expect large numbers of bacteria within these floating biofilms to survive addition of many different types of antibiotics. These results suggest reasons for the difficulty in eradicating established joint infections. They also suggest that the choice of antibiotics for peri/post-operative prophylaxis may need to be re-examined.”
“These floating biofilms can be induced to be antibiotic susceptible if they can be dispersed…conversely, if the aggregation can be inhibited, the bacteria in the synovial environment would regain some degree of antibiotic susceptibility. Our future research on this topic is aimed at creating new therapies that can aid in the disruption of these aggregates to restore full antimicrobial susceptibility.”
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.