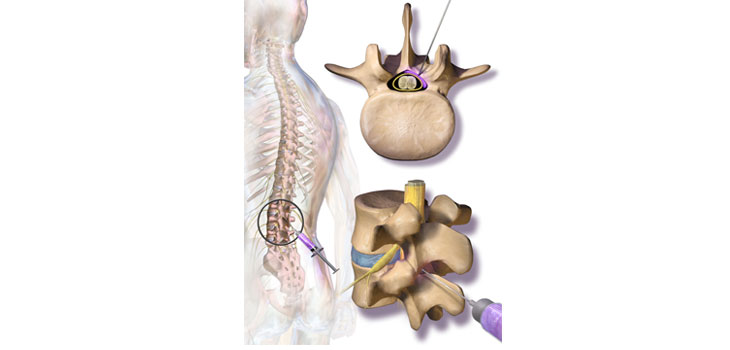
Patients with spinal stenosis who received epidural injections with a combination of steroid (glucocorticoid) and local anesthetic (lidocaine) did not improve any better than patients who only received lidocaine injections.
Steroid Injections for Spinal Stenosis Fail Test
3 min read Premium comments
Secondary
Those are the findings of a new study led by Janna Friedly, M.D., a professor of rehabilitation medicine at the University of Washington. It was the largest randomized trial ever performed to evaluate the procedure comparing epidural injections containing a combination of the steroid and anesthetic with injections containing anesthetic only in patients who had lumbar central spinal stenosis and associated leg pain and disability. The findings were published in the New England Journal of Medicine on July 2, 2014.
Over 10 million epidural steroid injections are given for spinal stenosis each year in the U.S. and cost anywhere from $500 to $2, 000 per procedure. Many of the injections are required by insurers before surgery is allowed. Injections are cheaper than surgery and with insurers only insuring individuals for a limited period of time, it’s a good strategy to push the problem to the next insurer. Under the new healthcare law, that dynamic may change.
Andersson: “Serious Questions”
In an accompanying editorial, Gunnar Andersson, M.D., Ph.D., president of the International Society for the Advancement of Spine Surgery and chairman emeritus of orthopedic surgery at Rush University Medical Center in Chicago, wrote “Certainly, this study raises serious questions about the benefits of epidural glucocorticoid injections for spinal stenosis. In patients who nonetheless proceed with an epidural glucocorticoid injection, repeat injections should be avoided if there is no effect.”
Dr. Andersson also noted that a January 2013 review and recommendation statement by the North American Spine Society (NASS) concluded that “there is insufficient evidence to make a recommendation for or against the efficacy of transforaminal epidural steroid injections in the treatment of lumbar radicular pain in the setting of foraminal stenosis” or “in the setting of central stenosis.” Similarly, a recent Cochrane review of nonsurgical treatment for spinal stenosis with neurogenic claudication concluded that supportive evidence for glucocorticoid injections was limited to “low-quality evidence.”
Baker: “Probably Won’t Work”
In a New York Times article, Ray Baker, M.D. a past president of NASS and the International Spine Interventions Society said the study provides evidence to tell some patients, “This probably isn’t going to work very well for you.” And because some participants received two injections without greater benefit, “it strongly speaks against the practice of performing multiple injections.”
Every patient received injections, and both groups reported similar improvement six weeks later, so there is no way to tell if patients would do as well without any injections at all. Also unclear is whether the anesthetic did anything helpful when injected alone. Some experts said the benefits patients reported seemed larger than typical placebo effects.
“To me it’s unlikely that the lidocaine has a long-term effect, ” Dr. Friedly told the New York Times, “but there are people who think that it could.”
The study also did not represent all types of stenosis, involving patients with central stenosis, not stenosis on one side, which Dr. Andersson noted in his editorial was more localized and therefore possibly more treatable by injection.
“On the basis of the largely negative results of the present trial and the lack of other rigorous data to support the use of glucocorticoid injections in these patients, I will remain cautious in prescribing epidural glucocorticoid injections for patients with lumbar spinal stenosis. Patients should be informed that the current best available data have not provided support for a clinically significant long-term benefit overall and that complications are possible, ” concluded Dr. Andersson.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.