SafeWire, LLC, a medical device company focused on the design and development of devices for minimally invasive spine surgery, announced today that it has received 510(k) clearance from the U.S. Food and Drug Administration (FDA) to market its Y-Wire 2 orthopedic guidewire with additional claims.
SafeWire Receives 510(k) Clearance for Y-Wire 2
1 min read Premium comments
Secondary
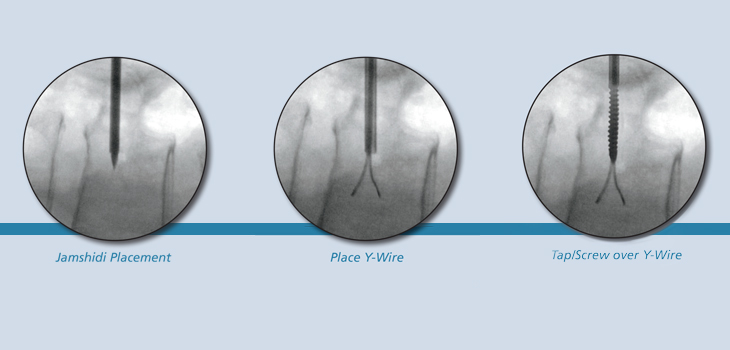
The Y-Wire 2 is a patented orthopedic guidewire with a distinctive split tip that is designed to prevent inadvertent advancement of the wire through bone. Upon exiting its delivery mechanism, the Y-Wire 2’s distal tips deploy to prevent further advancement.
Wyatt Geist, CEO of SafeWire said in the May 30, 2014 news release, “SafeWire is committed to the advancement of minimally invasive instrumentation for spine surgeons and their patients. FDA clearance of the Y-Wire is a significant milestone, and we are excited to provide the surgical community with a guidewire designed to mitigate inadvertent advancement during minimally invasive spinal surgery.”
Joseph Zavatsky, M.D., stated, “The Y-Wire 2 provides a solution to an ongoing issue in minimally invasive spine surgery. More importantly, it may also facilitate a return to bi-cortical fixation in the sacrum. Bi-cortical fixation in the sacrum has been the standard in open spinal surgery, but its adoption in minimally invasive surgery has been hampered by the issue of guidewire advancement.”
The Y-Wire 2 was designed for compatibility with a wide variety of delivery systems such as fluoroscopy, robotics and image guidance making adoption of this innovative technology less disruptive to hospitals with established instrumentation providers.
Asked about the product development phase, Geist told OTW, “It was important to be able to differentiate ourselves from all other guidewires.”
Asked where he hopes to be in one year with this product, Geist told OTW, “It might be best to just say that we will sell over 20, 000 Y-Wires in 2014 alone. We will plan for a larger percentage of the market with a deployment of our own cannulation products or potential licensing deals.”
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.