If you are a surgeon who works for a hospital, your pay depends on your employer maximizing all the reimbursements they can get from public and private sources.
20 States Turn Down Billions of Obamacare Dollars
2 min read Premium comments
Secondary
What if you found out that your hospital administrator was turning down federal reimbursement funds to pay for poor patients who show up at your doorstep? Worse yet, what if you found out it was politicians in your state who are keeping your administrator from accepting those funds already earmarked for you?
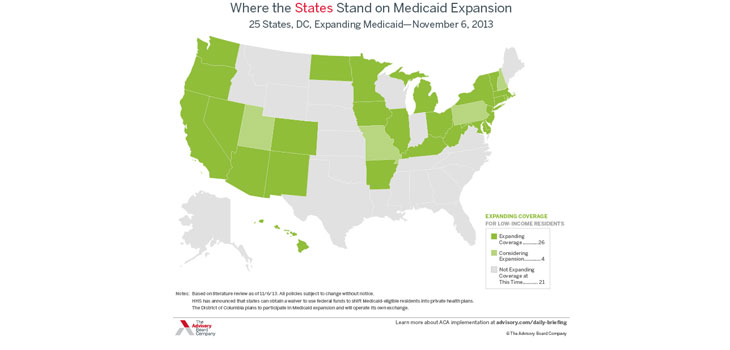
According to a recent study by the Commonwealth Fund, Texas hospitals will forgo $9.2 billion in federal funds over the next eight years. Florida is giving up $5 billion. Georgia, Missouri, North Carolina and Virginia will turn down over $2 billion; Louisiana, Oklahoma and Wisconsin, over $1 billion. Tennessee and Indiana are still deciding, but if they pass on the money, they’ll forgo more than $2 billion. Overall, 20 states have chosen not to take the money.
The money they’re turning down are funds already collected under Obamacare and designated to pay for the cost of expanding Medicaid coverage in the states. The rub is that citizens of those states will already have paid the Obamacare tax AND already pay for the care of the indigent. They’re putting taxes into the federal kitty, but refusing to take any of it back.
The political leaders of those states say they don’t want to get obligated to expanding coverage for the poor and that it will strain their state budgets after the federal subsidies run out. The federal subsidies will pay for 100% of the expansion for the first three years and then drop down to 90% thereafter.
Hospitals in those states are urging their state politicians to take the money. After all, it’s good economic development policy. For example, by 2022, Kentucky will spend about $1.7 billion in economic development incentives to attract new businesses. In that same time, the state will spend $301 million to cover additional low-income resident. Kentucky will receive $2.6 billion because it joined up.
Plus, the hospitals need the money. In some cases, hospitals have even agreed to pay new state taxes if their state leaders take the federal dollars because they expect their uncompensated care costs to decrease considerably.
“States that choose to participate in the Medicaid expansion will gain considerable new federal funds, ” the study’s authors write. “States often seek to increase their share of federal funds, lobbying for military bases, procurement contracts, and highway funds. Federal funding provides direct benefits and bolsters local economies.”

Taxpayers in states that don’t expand their Medicaid programs will still be on the hook for federal taxes aimed at covering costs in other states, without benefiting on their own, the authors conclude. And no state that rejects Medicaid expansion will actually save money, the report alleges.
Medicaid expansion will constitute an increasing share of federal funds allocated to the states in coming years. On average, the amount of new federal funds flowing to states that expand Medicaid will be more than twice as large as the amount of federal highway dollars by 2022.
If every state expanded Medicaid, the new program would cover up to 21 million Americans who make less than 138% of the federal poverty level.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.