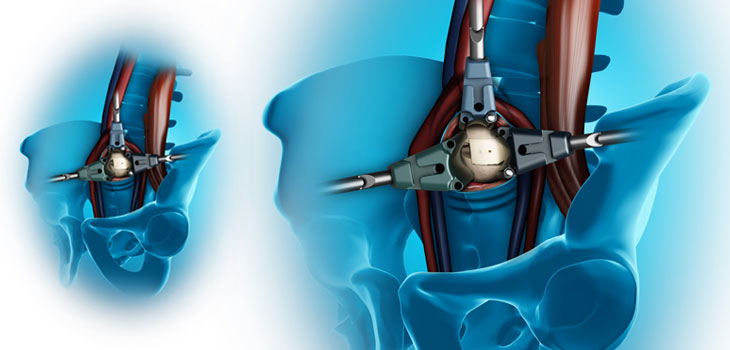
Medtronic, Inc. says it has scored a first by introducing the first procedure that allows lateral access to the most common operative level of the spine. According to an October 21, 2013, announcement, the OLIF51 procedure enables reproducible lateral access to the L5-S1 disc space.
Medtronic Claims “First” in Lateral Access Spine Surgery
1 min read Premium comments
Secondary
“For the first time, along with the OLIF25 Procedure, the surgeon community has a combination of procedures that offer an extensive approach to all levels of the lower lumbar spine in one patient positioning, ” said Richard Hynes, M.D., spine surgeon at The B.A.C.K. Center in Melbourne, Florida.
Referred to as Oblique Lateral Interbody Fusion for L5-S1, this procedure, says the company, eliminates the need to reposition the patient during surgery and incorporates Medtronic’s comprehensive surgical platform of access, interbody, neuromonitoring, navigation, fixation and biologic options, ” said stated the announcement.
Doug King, Medtronic Spine’s president and Medtronic senior vice president, said, “With the launch of the OLIF51 Procedure, Medtronic has aligned with expressed needs from the global surgeon community for procedures that require less muscle disruption and enable greater intraoperative efficiencies.”
The OLIF25, which was introduced at last year’s annual meeting of the North American Spine Society, targets the L2-L5 region of the spine, which is a slightly smaller range of the lumbar region than reached by the OLIF51.
Lateral Access Benefits
According to Adam S. Kanter, M.D., of the University of Pittsburgh, traditional posterior fusion techniques require the dissection and retraction of back muscles, bones, vessels, ligaments, and nerves; whereas traditional anterior approaches through the abdominal musculature risk injury to major vascular structures such as the aorta and iliac vessels, as well as the very delicate genitourinary structures. The lateral transpsoas approach enables the means to reproducibly address spinal pathology from the side of the patient, (utilizing novel dynamic real-time nerve localizing and monitoring techniques, thus minimizing surrounding tissue trauma and maximizing safety and efficacy.
The announcement was made during the annual meeting of the Congress of Neurological Surgeons in San Francisco, California.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.