Researchers from several universities in Taiwan have just published work showing that rheumatoid arthritis (RA) significantly increases the risk of potentially fatal blood clots in the legs and lungs. The study, which was done throughout Taiwan, was published online in the Annals of the Rheumatic Diseases.
RA Increases Risk of Blood Clots
1 min read Premium comments
Secondary
The team tracked the health of most of the population of Taiwan (23.74 million people) through the country’s compulsory national insurance scheme between 1998 to 2008, and included a further monitoring period up to the end of 2010. Just fewer than 30, 000 people developed RA during this period, and their details were entered into a national registry of the National Health Insurance Database (NHIRD). By way of comparison, they were matched with almost 117, 000 healthy people of the same age and sex. Three quarters (77%) of those who developed rheumatoid arthritis were women, and the average age at diagnosis was 52. Around one in five were over the age of 65.
Patients with rheumatoid arthritis were more likely to have other underlying conditions, such as high blood pressure, diabetes, high cholesterol, heart failure and fractures, than were those in the comparison group. But even after taking account of these influential factors, and allowing for age, patients with rheumatoid arthritis were still significantly more likely to develop potentially fatal blood clots, the analysis revealed.
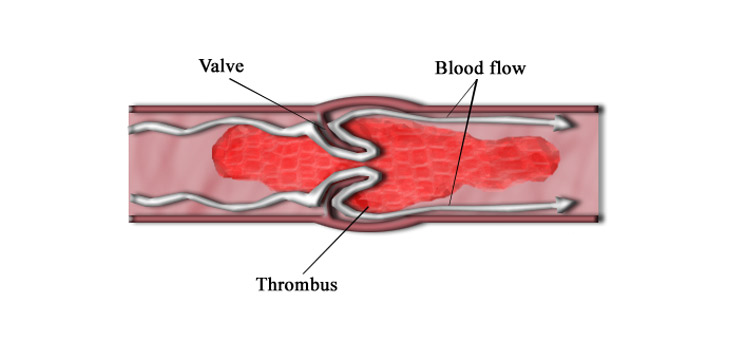
RA patients were more than three times as likely to develop a deep vein thrombosis (DVT), and twice as likely to develop a PE as those without the condition, the figures showed. Those RA patients under the age of 50 were almost six times as likely to develop a DVT and more than three times as likely to develop pulmonary embolism than were either middle aged (50 to 65) or older adults.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.