Benvenue Medical, Inc. just completed its 12-month follow-up on patients in the company’s KAST clinical trial.
Kiva Meets Clinical Trial Endpoint
2 min read Premium comments
Secondary
The results? The company announced on May 21, 2013 that the study ended early because the trial met the pre-determined stopping rules (non-inferiority).
Next Stop: FDA
The KAST (Kiva System as a Vertebral Augmentation Treatment – A Safety and Effectiveness Trial) clinical trial was conducted to support a 510(k) application for market clearance from the FDA, which the company expects to submit in the third quarter of 2013.
Sean Tutton, M.D., FSIR, co-principal investigator of the study and professor of radiology and surgery at the Medical College of Wisconsin in Milwaukee said, “We anticipate the results will be important to guiding treatment recommendations for VCFs.” Benvenue’s CEO, Robert Weigle, said the company is having a “positive collaboration with the FDA on our progress. KAST met the pre-determined stopping rules for enrollment completion and also enrolled ahead of schedule. Lastly, 98% of eligible patients were followed out to one year.”
Kiva vs. Kyphoplasty
The trial evaluated the Kiva Vertebral Compression Fracture (VCF) Treatment System in one of the largest, according to the company, randomized studies to date versus the current standard of care in the treatment of VCFs—balloon kyphoplasty. The primary endpoint was non-inferiority on a composite of pain, function, and safety at one year of follow-up on patients treated in the study. Three hundred patients were enrolled at 21 medical centers in the U.S., Canada, Belgium, France and Germany.
The study was designed to evaluate superiority on key secondary endpoints including PMMA (polymethyl methacrylate) cement volume, extravasation rate, and height restoration as well as other endpoints.
Kiva System
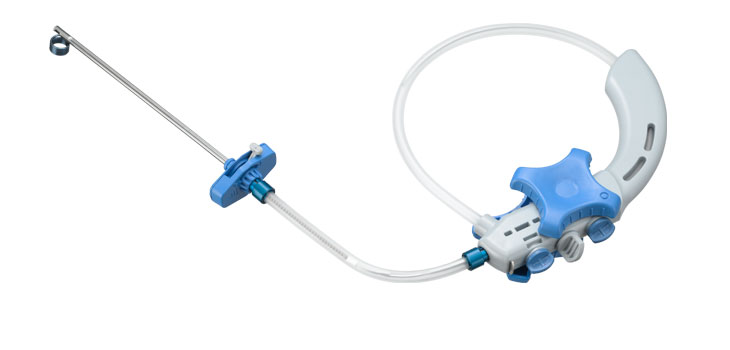
According to the company, the Kiva system features a proprietary flexible implant made from PEEK-OPTIMA, a biocompatible polymer. The implant is designed to function as a mechanical support structure and a reservoir to direct and contain the flow of bone cement.
The implant is delivered percutaneously in a continuous loop into the vertebral body through a small diameter, single incision. The amount of the implant delivered can be physician-customized during the procedure to adjust to various fracture types. Delivered over a removable guidewire, the implant is designed to provide stabilization and structural support to the vertebral body and to directionally control and contain bone cement.
A separate European randomized trial of Kiva and balloon vertebral augmentation was recently published in the February edition of Spine (2013;38:292-299). This Level I data, says the company, demonstrated Kiva’s superiority over balloons in key areas:
- Significant restoration of the Gardner angle in patients treated with Kiva ( p=0.002) whereas balloon kyphoplasty did not meet significance (p=0.067)
- Lower cement extravasation rates (3% for Kiva and 9.8% for balloon kyphoplasty, p<0.05)
- Lower cement volume (1.8 mL for Kiva and 2.8 mL for balloon kyphoplasty, p <0.001)
The National Osteoporosis Foundation estimates that there are 700, 000 osteoporosis-related vertebral compression fractures annually in the U.S. alone, yet 200, 000 kyphoplasty procedures are done globally.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.