A research team consisting of four Harvard professors, a researcher from the National Committee for Quality Assurance and L. Gregory Pawlson, from the Blue Cross Blue Shield Foundation, found that Medicare Advantage (MA HMO) plans may be offering more efficient patient care than do Medicare Part A and B plans.
Medicare Advantage More Efficient
2 min read Premium comments
Secondary
As reported by Anthony Brino, in Health Care Finance News, the team found MA HMO enrollees had 25% to 35% fewer emergency department visits, compared to traditional Medicare enrollees, and had 20% to 25% fewer inpatient medical days. MA HMO plans also had fewer ambulatory surgeries and procedures than in traditional Medicare, with ambulatory utilization 25% lower in 2003, before narrowing to 7% by 2008.
The authors studied rates of medical and surgical hospitalizations, outpatient visits, ambulatory procedures, emergency department visits and 12 specific surgical procedures, and compared MA HMO plans to Centers for Medicare and Medicare Services (CMS) enrollment and claims data from a random sample of traditional Medicare beneficiaries, adjusted for demographic factors.
According to Brino, inpatient surgical days initially were lower in MA HMOs, but by 2007 they had started to mirror traditional Medicare rates. HMO outpatient visit rates were also about 10% lower in the mid-2000s, before converging by 2009. Rates of elective knee and hip replacements were about 10% lower in Medicare Advantage HMOs for existing plans and were almost 20% lower for new plans after 2007.
The findings suggest that MA HMOs “may be able to treat a given patient with greater efficiency while attaining equal or superior quality through their flexibility in enrollee benefits, network contracting and coordination of care.” The team compared data from MA HMO and traditional Medicare plans from 2003 to 2009.
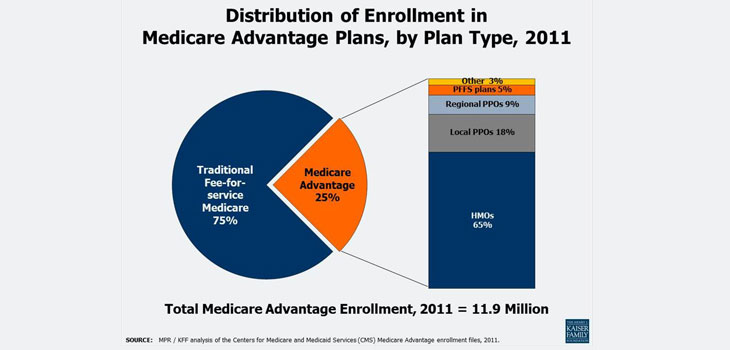
Brino reported that about a quarter of all Medicare beneficiaries, or 12.8 million, are enrolled in MA plans, up from 4.6 million a decade earlier. HMOs now account for 65% of MA enrollment. In 2003 the Medicare Modernization Act increased payments to participating plans that “made the program more attractive to beneficiaries because competition among plans and regulations led plans to pass along most of the extra payments to beneficiaries in the form of enhanced benefits or lower premiums, ” the authors wrote.
This first national analysis of MA HMO plans comes amid what Brino called booming enrollment in Medicare, an increase in Medicare Advantage enrollment and also concern for fixing Medicare’s cost and spending problems. The Department of Health and Human Services recently announced that MA plans are projected to increase enrollment by 11% in 2013 and that average premium prices will remain unchanged. Since 2010, MA premiums have decreased an average of 10% and enrollment in these plans has increased by 28%.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.