Using regional anesthesia rather than general anesthesia reduces the need for blood transfusions in patients undergoing bilateral total knee arthroplasty (TKR), according to a study at Hospital for Special Surgery (HSS) in New York City. The study appears online ahead of print in the journal Regional Anesthesia and Pain Medicine.
Regional Anesthesia Preferred for Bilateral TKAs
2 min read Premium comments
Secondary
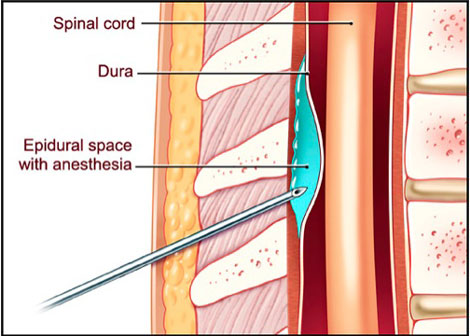
Currently, doctors perform the majority of bilateral knee replacements in the United States (as well as single knee replacements) under general anesthesia. Researchers at HSS say that a regional anesthesia known as neuraxial anesthesia should be promoted instead of general anesthesia for these procedures. Neuraxial anesthesia involves injecting medication into the fatty tissue that surrounds the nerve roots in the spine (known as an epidural) or into the cerebrospinal fluid that surrounds the spinal cord.
For the last two decades, HSS has increasingly used regional anesthesia for orthopedic procedures, because of a growing body of evidence showing favorable results compared with general anesthesia. For the study researchers compiled data from 40 acute care hospitals located throughout the United States. The study population included 22, 253 patients, but the type of anesthesia used was unclear in 6, 566 of the patients. Of the 15, 687 patients where anesthesia type could be identified, 6.8% received neuraxial anesthesia, 80.1% received general anesthesia, and 13.1% received a combination of both. The three groups had similar comorbidities.
The investigators discovered that patients receiving neuraxial anesthesia were less likely to receive blood transfusions (28.5%) than patients receiving general anesthesia (44.7%) or the combination (38.0%). They also identified a trend toward a reduction in major complications, such as pulmonary embolism and mechanical ventilation, with the use of neuraxial anesthesia compared with the other two groups, but this was not statistically significant. It is possible that, with only 1, 066 patients receiving neuraxial anesthesia, the sample size was too small to find other differences in complication rates.
“The use of neuraxial anesthesia may not always be feasible in every patient, but it should be considered more frequently, ” said Stavros Memtsoudis, M.D., Ph.D., director of Critical Care Services at (HSS) who led the study. “There is a lot of education that needs to be done in terms of training residents and orthopedic surgeons to point out the impact of the choice of anesthetic technique on outcomes beyond the operating room.”
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.