They are rare, but deadly. Bone and soft tissue sarcomas don’t appear in your average orthopedist’s office every day. And yet, if misdiagnosed—unlike most orthopedic conditions—they can result in death.
Sarcomas: What Do You Know?
8 min read Premium comments
Dr. James Wittig, Chief of Orthopedic Oncology and Associate Professor of Orthopedic Surgery at Mount Sinai Medical Center in New York City, does see these virulent conditions every day. And he wants his non-orthopedic oncology colleagues to know more. “I would like for the general index of suspicion to be higher for bone and soft tissue sarcomas. Why? Because I have many patients appear in my office who have not had a diagnosis made for months.”
Many of these patients have been told that they have a hematoma, a pulled muscle, or some type of sports injury. These cancers are nuanced and can definitely present as something similar to an injury.
A young athlete shows up at an orthopedist’s office complaining of thigh pain. Her physician examines her and says, ‘You just played a tough game. Ice it down, rest up, and you should be fine.’ “Maybe”, says Dr. Wittig. “Actually, patients with bone sarcoma usually complain of a mild ache in the area of the tumor that is often worse at night. And yes, many of these patients are between the ages of 10 and 20 and are involved in sports. Given this profile, an orthopedist may not order an X-ray because he thinks it’s a strained muscle or ligament. What complicates the decision making further is that even if an X-ray is ordered, it may still be negative since tumors grow so rapidly that they don’t cause visible (on an X-ray) destruction of the bone. The tumor is then ultimately identified by the physician on an MRI—maybe six months later. It is important for physicians to see their patients back in the office six weeks after they sustain an injury or complain of an area of pain. If the pain persists then an X-ray and MRI are indicated.”
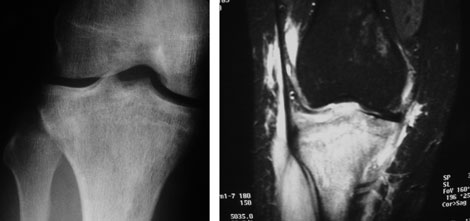
 This is a patient who gave a history of 6 months of pain in her knee. She had seen multiple doctors who examined her and obtained X-rays. X-rays were negative and she was diagnosed with a strain. Finally the pain persisted and she began to develop swelling. An MRI was ordered that demonstrated a malignant tumor arising from the proximal tibia.
This is a patient who gave a history of 6 months of pain in her knee. She had seen multiple doctors who examined her and obtained X-rays. X-rays were negative and she was diagnosed with a strain. Finally the pain persisted and she began to develop swelling. An MRI was ordered that demonstrated a malignant tumor arising from the proximal tibia.
The x-ray is virtually normal. The lesion is extremely permeative resulting in only very subtle changes on the Xrays that were retrospectively identified after reviewing the MRI. The MRI clearly demonstrates the tumor.
Teasing out a bone sarcoma from a soft tissue sarcoma can usually be done by evaluating the patient’s pain level, says Dr. Wittig. “Patients in the early stages of bone sarcoma usually present with a dull aching pain that is persistent and may worsen with activities (causing some doctors to think it is a mechanical problem). This is because the tumor is growing and causing swelling around the bone. This is in contrast to soft tissue sarcomas where the tumor is growing from a muscle or in the soft tissue between the muscles; it may be malignant, but it is painless. Because it is painless the physician misses it, it grows significantly and is ultimately diagnosed using an MRI. Some of these masses may be soft and subcutaneous and may even palpate similar to a lipoma, a common benign fatty tumor, and be missed by the orthopedist.”
“Flu like symptoms” are one thing you won’t hear from a sarcoma patient, says Dr. Wittig. “A lot of doctors think that these patients might have fever, weight loss, or night sweats, but that is not so. We must look elsewhere for clues. Unfortunately, even an X-ray might not give us information as a patient can have a tumor develop in the bone that doesn’t show up on an image. With bone sarcoma the pain may or may not be relieved by medication, and may involve night pain, an ominous sign that physicians want to look out for. I generally tell my patients that if the pain or swelling doesn’t disappear in six weeks to come back and see me and get an MRI.”
As so often happens in medicine, you look in one direction and find something pointing in another. Dr. Wittig: “Sometimes patients have radiological studies for other problems like a rotator cuff issue and a mass is incidentally identified on the radiological. We biopsy it and it turns out to be sarcoma.”
“On other occasions, ” says Dr. Wittig, “patients present with a mass in the thigh or leg, it is diagnosed as a blood clot, and they are sent for Doppler imaging. If there is significant hemorrhaging in the tumor patients can be diagnosed as having a hematoma. While certain tumors resemble a hematoma on an ultrasound or MRI, a hematoma will usually improve within six weeks.”
While your average radiologist may be very skilled, he or she doesn’t likely see many sarcomas crop up on imaging. “In the case of bone sarcoma, some patients in the early stages present with the appearance of a benign tumor, something more likely to be misread by a radiologist not experienced with tumor studies. For example, I had a patient who was playing soccer and tore her ACL. She also had a small lesion in the femur that was read as benign on an MRI. After being followed for several months, the lesion grew and was finally determined to be malignant. The child ultimately underwent an amputation. The key is to always question yourself and to have a high index of suspicion. Small lesions in bone may appear benign and require close monitoring by an orthopedic oncologist.”
Then there are patients who are fortunate enough to see someone who has heard Dr. Wittig’s message. “I recently had a young patient who was in a car accident and had a pelvic injury to her left side. The treating orthopedist fixed her pelvis, but in the process of reviewing the X-rays noticed a lesion on the opposite side of her pelvis. While it appeared benign, the orthopedist—who had trained with me—went the extra step and ordered a CT scan and a bone scan. He then sent the patient to me for a biopsy and it turned out to be the smallest Ewing’s sarcoma I had ever seen in bone.”
In the cacophonous, high tech world of medicine, it pays to be a little old fashioned. “Listen to your gut. If things don’t add up, you may be looking at a tumor. If the person has injuries or fractures to the bone you should think about the mechanism of injury. I recently had a kid who was fine during his baseball game then fractured his femur while walking off the field. The X-rays didn’t reveal a tumor and the fracture hematoma made it difficult to interpret the MRI but we did a biopsy and found a sarcoma growing in the bone. Extreme care is required when going after these tumors, as you can sometimes go in and disrupt the sarcoma. If you open up the fracture site where the tumor is growing and you put a metal rod through the area, then that will cause the tumor to spread and the patient will most likely require an amputation. Again, be suspicious that what you are looking at is actually what you think it is.”
Dr. Martin Malawer, Professor of Orthopedics at Georgetown University School of Medicine, completely agrees. “Be wary if a young or middle aged adult shows up in your office with a painless mass—that could very well be a soft tissue sarcoma. The tendency is to think that if the person is young then they have been involved in a trauma, with around 40% of patients saying that they fell, bumped their shoulder, etc. An old time cancer surgeon would call that ‘traumatic determinism, ’ i.e., the act of falling or bumping into something brings attention to the mass. Anything larger than a few centimeters should immediately be considered malignant.”
A big purple bruise naturally draws attention. But, says Dr. Malawer, dig deeper. “If someone has fallen or bumped themselves, doctors will say, ‘It’s likely a hematoma.’ The problem with this is that a hematoma rarely occurs after trauma to the muscle. The best course of action is to get an MRI, because the signal sequences can tell you if it’s fat or not and if it’s solid, homogeneous, or heterogeneous. An MRI will also let you know if it is necrotic or blood filled, the latter being a sign of a high grade malignancy.”
Then there is the issue of how to retrieve the cells for examination. “In the past surgeons would remove part of the tumor and figure out what it is afterwards. Now the standard of care is to do a core biopsy, going to the core of the tumor. What should not be done is a fine needle aspiration because they are hard to work with and most pathologists don’t have lot of experience with them. You also want to avoid an incisional biopsy whenever possible because cutting into the tumor will make it bleed and cause the wider area to be contaminated with tumor cells.”
Then, Dr. Malawar notes, there are risks associated with relying on a non-specialist to handle such oncological issues.
For example, there are even 135 tumors of the foot and ankle. This is certainly not an area where you should do an incision and take something out if you’re not sure because it’s not an area where there is room for error.
Homing in on bone sarcoma, Dr. Malawer notes, “There are two groups of these cancers, one of which occurs in peds and adolescents. These cases are best treated in specialty centers with a multidisciplinary team that knows how to approach the biopsy. As Dr. Wittig mentioned, 20 years ago we would make a hole, clean out the area to get a look, and then figure out what it is we were dealing with. This was when the only treatment was amputation; today 95% of cases of bone sarcoma in kids result in limb sparing surgery. One of the major reasons we’ve changed our approach is to avoid massive contamination from an inappropriate biopsy. In our practice the radiologist always asks me where exactly to do the biopsy…in fact, he wants me to put an X on the spot.”
These toxic sarcomas also strike individuals in another category, says Dr. Malawer…those over 45 years of age. “These are chondrosarcomas and tend to occur around the pelvis or shoulder girdle. They are complex because they can mimic almost anything and can involve buttocks pain, sciatica, pelvic pain, etc. Patients might waste valuable time going, for example, to the OB/GYN before finally ending up with an orthopedic oncologist.”
Soft tissue sarcomas are serious for people in any group, ” states Dr. Malawer, “but they are one of the more common causes of death in young people. Whatever you do, don’t let your guard down if someone shows up in your office with any of the aforementioned symptoms.
React:
Discussion
This is a fascinating development. In my practice we've seen similar outcomes with the revised protocol. The key differentiator seems to be patient selection criteria. Has anyone else noticed the correlation with BMI thresholds?
Great point. I'd push back slightly on the conclusion, the sample size in the cited study is too small to draw population-level inferences. That said, the directional signal is compelling and worth a larger RCT.
We implemented a similar approach last year. Early results are promising but we're still gathering 12-month follow-up data. Happy to share our protocol if anyone is interested.
Join the conversation
Orthopedic professionals are discussing this. Sign in and upgrade to read every comment and add your voice.